
This is my first time participating in Diabetes Blog Week and I am overwhelmed at the idea of publishing a blogpost every day for seven days. I usually take a long time (too much time!) to write each blogpost and that just won’t be possible in this scenario. At least I had access to the topics a week ahead so that I could get a head start thinking and writing and thinking more and writing more and thinking a lot more and …. Well, you get the picture. Thanks to Karen Graffeo of Bitter~Sweet™ for being the brains behind this project and organizing it for the fifth year.

Today’s Topic: Let’s kick off Diabetes Blog Week by talking about the diabetes causes and issues that really get us fired up. Are you passionate about 504 plans and school safety? Do diabetes misconceptions irk you? Do you fight for CGM coverage for Medicare patients, SDP funding, or test strip accuracy? Do you work hard at creating diabetes connections and bringing support? Whether or not you “formally” advocate for any cause, share the issues that are important to you.
 As I looked at the topics for this week, today’s subject is the hardest one for me to write about. In recent months, discussions about advocacy have been everywhere. In some ways I think I’ve already said it all. And if I haven’t said it, for sure someone else has. Unfortunately just because we’ve talked about issues over and over again doesn’t mean that the problems have been solved and we no longer need to think about them. No, the problems are still here and we need to keep bringing them back to the forefront.
As I looked at the topics for this week, today’s subject is the hardest one for me to write about. In recent months, discussions about advocacy have been everywhere. In some ways I think I’ve already said it all. And if I haven’t said it, for sure someone else has. Unfortunately just because we’ve talked about issues over and over again doesn’t mean that the problems have been solved and we no longer need to think about them. No, the problems are still here and we need to keep bringing them back to the forefront.
I think that there is an umbrella under which all of my advocacy concerns about diabetes fit. I strongly believe that everyone with diabetes needs access to proper care and supplies. That can mean a lot of different things. I participated in the Spare a Rose, Save a Child campaign in February. That was and is the nitty-gritty of needing proper care and supplies. Many children diagnosed with diabetes in developing nations have almost no access to education and insulin. Every donation to the campaign made a huge impact because a child who had absolutely nothing was given the gift of life.
Although insulin and diabetes supplies are more readily available in the United States than in developing countries, I would still argue that many people in our country are not getting proper care for their diabetes. Every person who is told that she has a “little bit of diabetes” and then sent home without education and test strips is not getting proper care. Every adult with crazy high blood sugar who is handed pills without any consideration that he might have Type 1 instead of Type 2 diabetes is not getting proper care. Every child who has the flu-like symptoms of diabetes at the pediatrician’s office and doesn’t get a routine blood glucose test is not getting proper care. Unfortunately these stories happen every day. Too many people with Type 2 diabetes are only diagnosed once complications have set in. Too many people with Type 1 diabetes are simply handed Metformin when their bodies are screaming for insulin. Too many children end up in the ICU with DKA or even die when a simple fingerstick at the pediatrician’s office might have diagnosed diabetes.
My co-blogger Sue from Pennsylvania has written extensively about the struggle to have Medicare cover the cost of a continuous glucose monitor (CGM) for her Type 1 husband. What was considered proper care for him when he was 64 years old is now considered “precautionary” and being denied now that he is 65. In addition, Sue’s husband and many other pump-users on Medicare are increasingly having problems finding vendors to provide their insulin under Part B because Medicare’s outdated reimbursement rates are less than the vendor’s cost to purchase the insulin. Medicare coverage needs to reflect current standards of care for diabetes and its reimbursement rates need to cover current costs for things such as insulin. Without those changes, many seniors with diabetes will continue to struggle to access the diabetes supplies and medications that keep them healthy and safe.
As someone who is living with Type 1 diabetes and getting older, I increasingly worry about receiving proper care once I am no longer able to care for myself. Whether it is a short hospitalization or a permanent move to a nursing home, I need my caretakers to understand the differences between the types of diabetes and treat me appropriately. I have been “privileged” to have good insurance throughout my diabetes life, but no amount 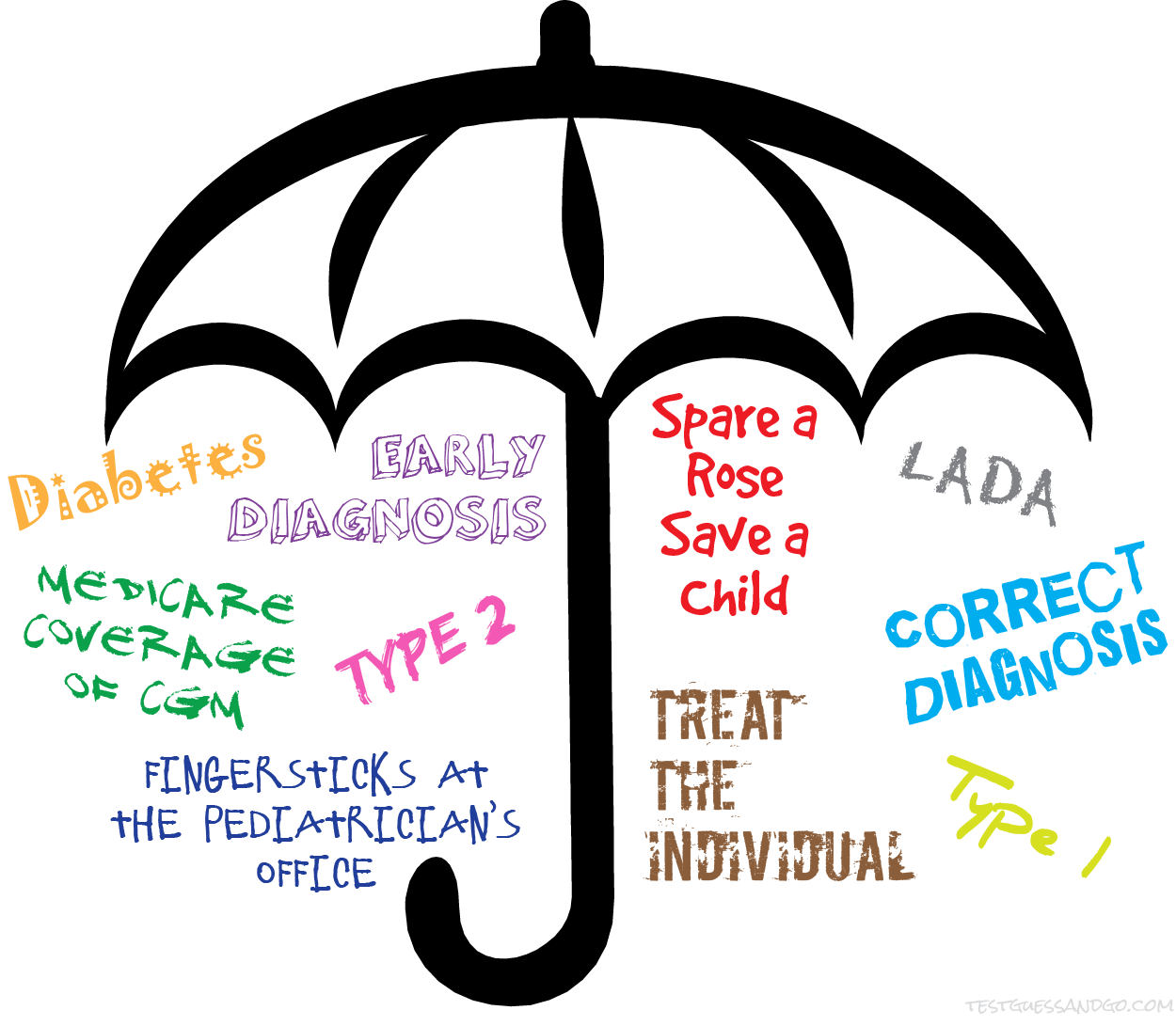 of privelege will protect me from a potentially lethal injection of insulin based on a Type 2 sliding scale. Proper care isn’t a sometimes thing. It needs to be an everyday thing for every individual with any type of diabetes.
of privelege will protect me from a potentially lethal injection of insulin based on a Type 2 sliding scale. Proper care isn’t a sometimes thing. It needs to be an everyday thing for every individual with any type of diabetes.
Proper care and access to supplies and medications. That’s a gigantic umbrella over a huge number of issues for people with diabetes. Until children in developing countries have reliable access to insulin, until people with Type 2 diabetes are diagnosed before complications have set in, until Medicare recipients with hypoglycemia unawareness have access to CGMS, until no child has to die of undiagnosed diabetes, until….
Until everyone with diabetes receives proper care and access to needed supplies and medications, our job is not done.











 Today I sent a letter to most of my friends and family members. It was easy for me to write
Today I sent a letter to most of my friends and family members. It was easy for me to write 
