
 I’ve been on a blogging vacation. It wasn’t intentional, but one missed post turned into another missed post. And another missed post. Before I knew it, my twice weekly postings had turned into none. Blogs aren’t supposed to be a burden, so I’m not feeling too guilty. Unfortunately my blogging vacation has been accompanied by a lapse in my diabetes care. A few (well, maybe a lot of) bad decisions along with infusion set problems have resulted in a series of days (weeks?) with less than optimal numbers.
I’ve been on a blogging vacation. It wasn’t intentional, but one missed post turned into another missed post. And another missed post. Before I knew it, my twice weekly postings had turned into none. Blogs aren’t supposed to be a burden, so I’m not feeling too guilty. Unfortunately my blogging vacation has been accompanied by a lapse in my diabetes care. A few (well, maybe a lot of) bad decisions along with infusion set problems have resulted in a series of days (weeks?) with less than optimal numbers.
My diabetes care is never perfect, but for the most part I do pretty well and spend a lot of time in my “target range”. For much of the last year I have had success with a low carb diet (most of the time) and an insulin regimen that has controlled my morning blood sugar spikes (most of the time). So what has thrown everything out of balance?
A little bit of this and a little bit of that.
Balance is the hardest part of Type 1 diabetes. Without a functioning pancreas, our bodies have no sense of equilibrium. We live on a tightrope where good numbers are a small step from catastrophic lows and higher numbers seem to send the glucocoaster spiraling out of control. It’s the reality that everything today is connected to everything yesterday and will influence everything tomorrow.
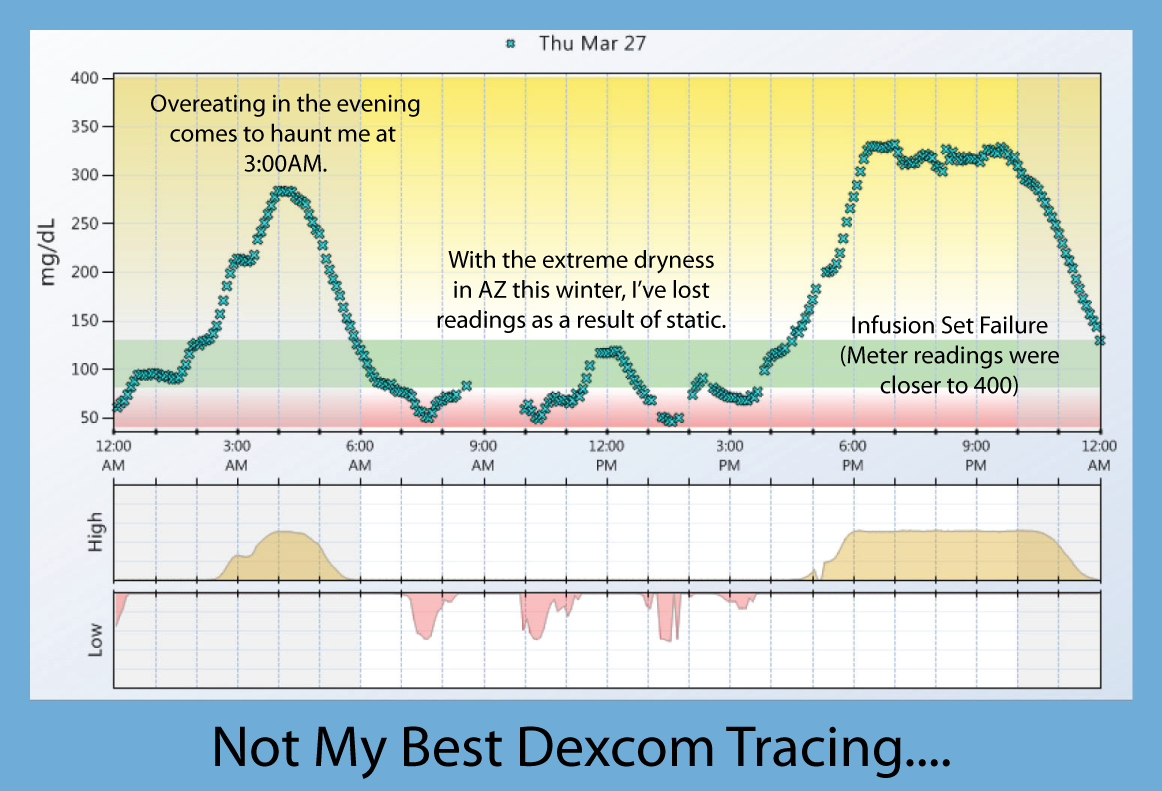
I eat a couple of chocolate chunk cookies. Okay, they are the (huge!) chocolate chunk cookies (delicious!) from Costco. I take a boatload of insulin and my BG numbers seem to stay in check. But at 2:00AM my Dexcom screams that my BG is high and rising quickly. I program a correction dose into my pump and unfortunately wake up with a low at 6:00AM. Two glucose tabs and before I know it, I’m back to 180 and rising quickly. I test frequently and take enough insulin to vanquish two plates of pancakes, a banana split, and half a loaf of Wonder Bread. But wait, I didn’t eat any of those things. I either ate nothing or my normal 17 carb breakfast of Greek yogurt and apple or blueberries. The dog walk that usually prevents huge post-breakfast BG spikes is rewarded with numbers in the 200’s.
My endocrinologist claims that overnight lows result in hormones that ultimately cause highs. I think she’s right because the more overnight lows I have, the more daytime highs I see. The more I correct the highs, the more I end up low. Dexcom tracings that resemble the Himalayas multiply rapidly and refuse to give way to somewhat gentler blood glucose slopes.
The cookies are long gone and the sweet, yummy, chocolaty taste is a pleasant guilt-laden memory. The problem is that my diabetes remembers the indiscretions and even when I’m eating a judiciously low-carb meal, my body is quick to spike and quick to crash. Add frustration and diabetes burnout to the mix and it’s hard to get back on the straight and narrow.
Mixed in with things I can control are things like infusion set failures. I have used angled sets (Silhouettes and Comfort Shorts) successfully for most of my pumping life. Skin problems, inflammation at pump sites, and insertion pain have motivated me to explore other types of sets. In my last supply order, I included a box of Insets and a box of Cleos. I started with the Insets and loved the pain-free insertion. Since I weigh a little more than the last time I used 90-degree sets, I was encouraged by the performance of the first 9 sets with no pain, no failures, and all of them lasting 3 days. Then came #10. It was a blast from the past with an absolute failure five hours after insertion. I rarely get insulin blockages with angled sets. This site failure reminded me why I had quit using Quick Sets ten years ago and learned to live with the horrible insertion needles of angled sets. I’ll use the box of Cleo’s and probably go back to Comfort Shorts. I can stand a little pain and inflammation to have reliable insulin delivery.
After covering a lot of subjects here without much sense of direction, I’ll wrap up by saying that I’m back to blogging after a brief hiatus. Judging from the last two days, I think my diabetes care is back on track. In many ways these two things go hand-in-hand because they are reflections of how much diabetes is like a spoiled child who demands all of our attention and won’t settle for less than 100%. Not even when you want a vacation….








