
I purchased my first Tandem X2 pump in December 2016. Shortly after that in April 2017 I transitioned to Medicare. Thus when my original pump went out of warranty in early December 2020, I was free to choose a new pump. I am sad that there are not more pump choices these days. I hated Omnipod and it is a poor financial choice under Medicare. I liked my Medtronic pumps ways back when, but I would never abandon Dexcom for Medtronic sensors. So it is Tandem again. I was not unhappy to continue with Tandem but I was sad to miss the excitement of a new D-device, because the new one is the same as the old one.
But not entirely.
I had the choice of purchasing a Tandem X2 pump with the Control IQ software or a Tandem X2 pump with the older Basal IQ software. So I chose Basal IQ and I am now in the unique position of being able to choose between Basal IQ and Control IQ depending on which pump I am using.

I have never been completely satisfied with Control IQ and chafe at target ranges that are higher than I prefer and significant insulin suspensions that result in highs later on. Basal IQ is much quicker to resume insulin after suspensions and I was excited to get back to it. Initially I was happy with somewhat better BG readings and more control over my pump behavior.
But after a month, I chose to go back to Control IQ today.
Why?
One of the reasons is minor. I really missed the automatic population of my sensor reading when I was bolusing. Somehow it has been a step backwards (okay, I am lazy!) to have to type in the number. Minor, but significant.
Another reason is that my initial excitement and honeymoon period with Basal IQ ended quickly and I wasn’t doing better with it than with Control IQ.
But mostly I missed the constant basal adjustments that Control IQ makes to tweak my blood glucose. (Please note that I use Sleep Mode 24/7 so I don’t get automatic boluses by Control IQ.) Because our infused insulin is slow, slow, slow, these adjustments don’t work as quickly as my impatient self would hope, but they do help. Control IQ gives me better and more consistent morning wake-up numbers. It also allows me to occasionally forget about diabetes when I hike and play golf.
I have never figured out “perfect” pump settings with Control IQ and previously took an injection of Lantus every evening to give me insulin that Control IQ couldn’t take away. https://testguessandgo.com/2020/09/25/going-untethered-with-control-iq/ That worked well but I have not missed the daily 7:30PM phone alarm beeping “Time to take a shot, Laddie!” So I am going to try to do without the untethered regimen, but that remains to be determined.
I have a history of my doctors thinking I am doing great regardless of my diabetes regimen. I was one of the last Type 1 patients to start Lantus because my world-renowned endocrinologist thought I was doing well on NPH. During the 2015 Blog Week (remember Blog Week?!?), I wrote that the biggest improvement in my diabetes care was the result of an internal medicine doctor switching me to Lantus. So much for world-renowned endocrinologists….
My Blue Ribbon First Place Change
That being said, I think that I am capable of getting the same A1c on injections, pumping without sensors, pumping with sensors, Basal IQ, and Control IQ. I truly believe that I am safer with sensors, but I can get reasonable BG numbers without them. Not completely true, because there would be some bad lows. But what I truly want is easier diabetes and that seems to be an elusive goal.
The biggest weakness in all of my regimens is “ME.” Imperfect me, who works hard at diabetes every day, but who constantly makes less than optimal decisions. Second glass of wine resulting in too many post-dinner cookies. Thinking there is a way to successfully bolus for pizza or Kraft Macaroni ’N Cheese. Buying a Diet Coke at a convenience store and being too lazy to check to see if it is really regular Coke. (It happened this week. A perfect flatline in the 90’s up to the mid-200’s in 20 minutes.) There is no end to the ways to screw up. And I am a master at thinking WTH as I muddle through my days.
But WAIT!!!
I am not perfect but the real culprit is TYPE 1 DIABETES. It is amazing how incredibly difficult it is to control blood sugar without a functioning pancreas. When I make good decisions, I get a bad pump site. I wake up at a good number and don’t do anything “wrong,” but my BG soars today while yesterday it stayed in target range. I am a senior with skin and tissue issues that sometimes rebel at infusion sets and adhesives. I am really smart and experienced, but sometimes I have no idea what is causing highs and lows. My lab tests confirm that my body makes zero insulin and this is hard.
I am very cognizant of the fact that the more my insulins and technology improve, the more I raise my expectations of what my diabetes numbers should be. So I am always falling short.
I think that once again I am writing about diabetes distress. My endocrinologist is very satisfied with my diabetes numbers. She believes that at my age (68) with 44 years of diabetes, my Dexcom tracings are perfect. And I am really, really, mostly, mostly okay. But I could do better.
By switching back to Control IQ, I am going to work to accept the help it gives me and not stress over the limitations of the algorithm. And the limitations of my insulin. And the limitations of my behavior.
My old pump has battery issues and ultimately I will have to decide whether to update the new pump to Control IQ. But right now I am happy to have CHOICE. I may choose to go back to Basal IQ on the new pump next week. I may choose to stay with Control IQ on the old pump.
I like choice.
Unfortunately one thing I don’t have choice about is having diabetes….
 I would love to say that I am doing fantastic things at home during the coronavirus crisis.
I would love to say that I am doing fantastic things at home during the coronavirus crisis.


 In April Diabetes Core Update released about 10 podcasts directly related to diabetes and the coronavirus. Although these podcasts are directed towards medical professionals, they contain the information that I as an engaged patient am starved for.
In April Diabetes Core Update released about 10 podcasts directly related to diabetes and the coronavirus. Although these podcasts are directed towards medical professionals, they contain the information that I as an engaged patient am starved for.




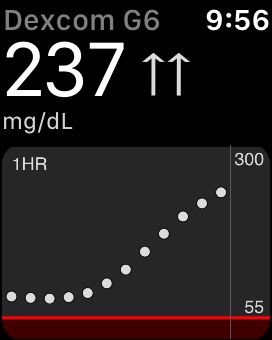
 with Control IQ. Many or most users have written on Facebook about making their settings much more aggressive. My initial days with Control IQ were rocky and I rarely had BG’s as low as the 110-120 range, even overnight. So I created a new pump profile titled “Aggressive.” And it was aggressively aggressive with high basals and correction factors that I had never previously used except when on steroids. Ultimately this aggressiveness was counter-productive because my basal insulin kept being reduced or suspended for long periods of time and that resulted in highs later on. This pump screen photo is an ugly result of too aggressive settings. My basals were reduced and suspended for almost 3 hours.
with Control IQ. Many or most users have written on Facebook about making their settings much more aggressive. My initial days with Control IQ were rocky and I rarely had BG’s as low as the 110-120 range, even overnight. So I created a new pump profile titled “Aggressive.” And it was aggressively aggressive with high basals and correction factors that I had never previously used except when on steroids. Ultimately this aggressiveness was counter-productive because my basal insulin kept being reduced or suspended for long periods of time and that resulted in highs later on. This pump screen photo is an ugly result of too aggressive settings. My basals were reduced and suspended for almost 3 hours.


 besides Caesar salad that I can eat there without bad BG results. I haven’t found it yet. Yesterday I had a bowl of Ten Vegetable soup. The posted carb count was 16 grams. I bolused for 35 grams in addition to a 200% temp basal that I had started 30 minutes earlier.
besides Caesar salad that I can eat there without bad BG results. I haven’t found it yet. Yesterday I had a bowl of Ten Vegetable soup. The posted carb count was 16 grams. I bolused for 35 grams in addition to a 200% temp basal that I had started 30 minutes earlier.




